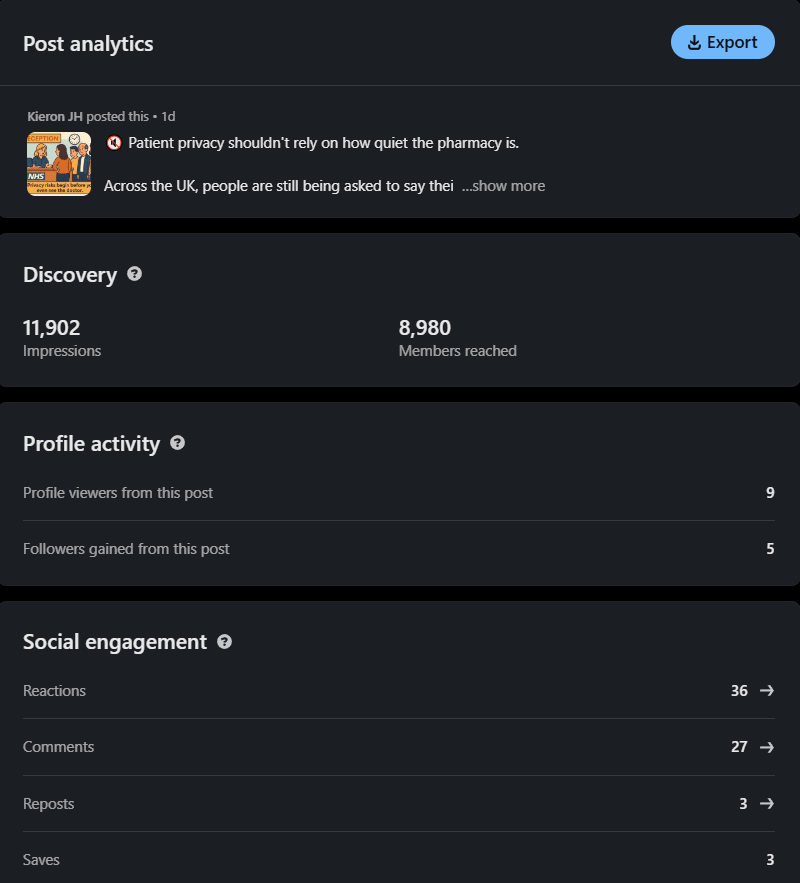
The follow up to our pharmacy and GP reception privacy piece. This time we build on what the public and professionals said in the discussion, and we move the argument forward.
Original article: NHS Pharmacy and GP Reception Privacy
Discussion thread: LinkedIn responses
What the first article covered, briefly
The first piece set out a simple reality. Many GP receptions and pharmacies still handle identity checks and handovers in public. Names, postcodes, exemption status, and sometimes what the medication is for are spoken within earshot of a queue. Spoken data is still personal data. Once heard, it is gone. This follow up does not repeat that ground. It builds on what the discussion exposed.
What the discussion added
Discretion is not a process
Several readers said their local site is respectful and quiet. That is good to hear. It is also luck. If privacy depends on who is on shift, there is no privacy. There is only chance.
Spoken information still counts
Privacy and compliance professionals were clear. Names and dates of birth are personal data even when spoken. Confidently calling full names and talking exemptions into a queue is a controllable risk that rarely gets logged.
Lived experience changed the room
One contributor with experience of privacy first healthcare described a normal handover in their home system. You hand over a card. Verification is quiet. No one in the queue hears anything. It works because privacy is the default, not because staff are unusually kind.
In my home country you never speak personal details aloud at a pharmacy. You hand over a card. Nobody in the queue hears anything.
They added why that matters. If you have moved address for safety, public recital is not a minor moment. If your medication could expose something personal, the exposure is not academic. That perspective humbled a few people who had framed this as oversensitivity. The tone shifted.
Low tech is fine
Another practical point landed. Use token numbers. Cheap and obvious. If a deli counter can avoid broadcasting identities, a healthcare counter can too.
People change behaviour to avoid exposure
Some readers avoid busy times. A few avoid collecting medication altogether. That is not a customer service quirk. That is a barrier to care created by design.
What this means in practice
This is not a call for marble screens or a national rebuild. It is a call for standards that remove exposure from a basic interaction.
- Default to numbers, not full names, when calling people forward
- Keep identity checks quiet at handover, not across a shop floor
- Offer a low friction private option and make it normal to use it
- Train counter staff in GDPR, safeguarding, and simple scripts that reduce blurting
- Fix counter layout where small changes prevent public recital
The accountability piece that makes it stick
If this is treated as etiquette, it will never stick. Treat it as governance.
- Record when spoken identity checks go wrong, as you would a dispensing error
- Measure whether exposure is falling, not only whether training was completed
- Offer a short form for anyone asked to speak personal details publicly, reply within one week
- Publish a short standard that any practice or pharmacy can copy, including numbers, scripts, quiet options
Why this matters now
Healthcare access should not depend on confidence, safety, English fluency, or emotional bandwidth. The current pattern assumes everyone is fine. The discussion showed how often that is false. People are not offended. They are exposed. Sometimes exposure is dangerous.
Closing thought
If other systems consider quiet identity handling as basic as turning the lights on, the UK can do the same. This is not innovation. It is catching up. One small change in process. One less moment where someone chooses between dignity and a prescription.

Be First to Comment