In 1981, two American researchers filmed people walking down a New York street and showed the footage to convicted violent offenders. They asked a simple question: who would you attack?
The offenders agreed with each other almost every time. And when asked how they knew, most of them couldn’t say. They just knew.
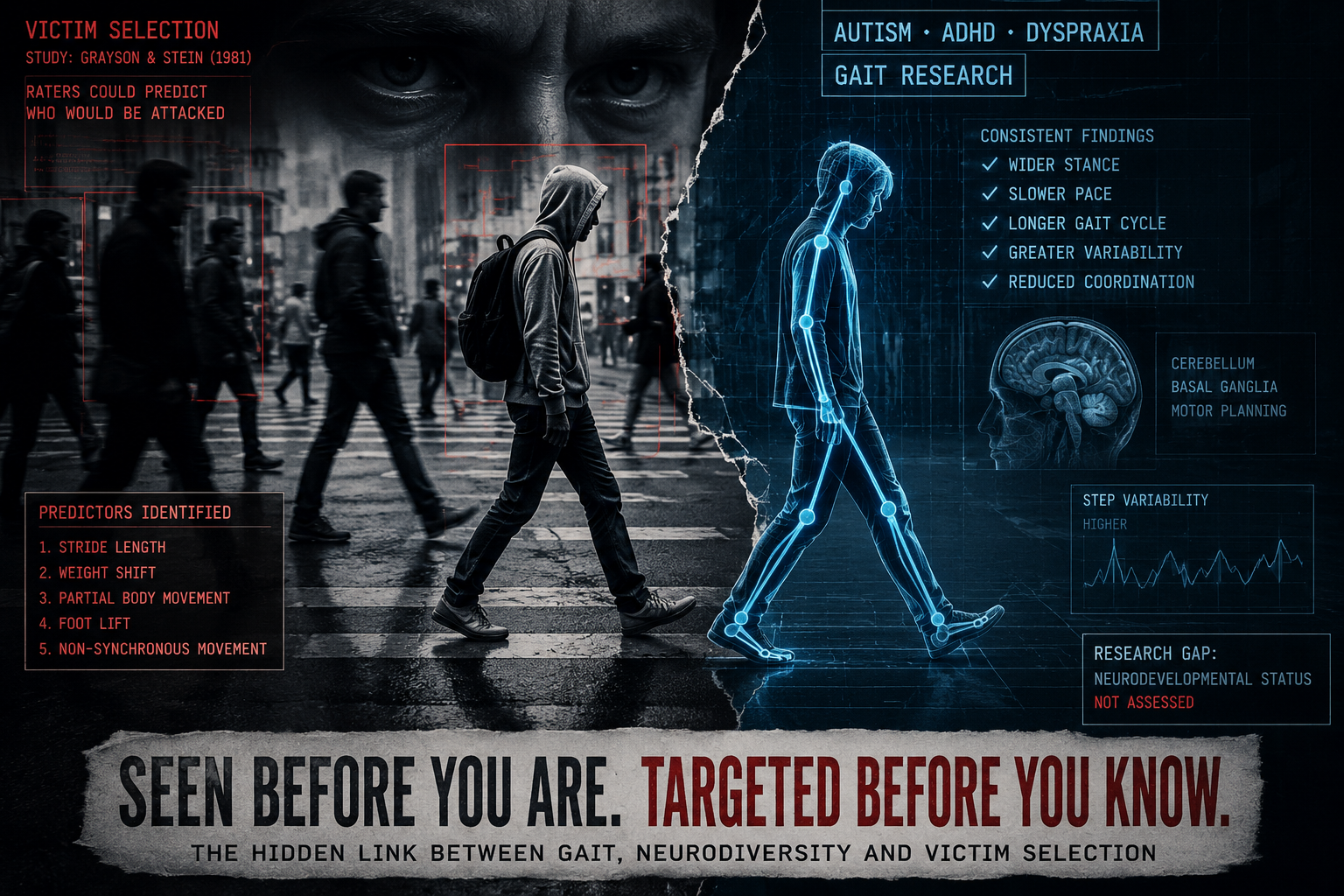
That study, by Betty Grayson and Morris Stein, has been quietly cited and replicated in criminology for over 40 years. It found that predators choosing a victim are responding to something specific and physical: the way a person walks. Not their size. Not necessarily their sex. Their gait.
What nobody in that field has asked, in four decades of follow-up studies, is what happens when you put that research next to a separate, equally well-established body of medical literature: the one showing that autism, ADHD and dyspraxia all produce measurable, often lifelong differences in gait.
The original study
Grayson and Stein’s method was simple. They filmed members of the public walking in New York, then had violent offenders rate each person on how easy they would be to attack.
The raters were consistent. Around half labelled the same individuals as easy targets, and the same individuals as ones they’d avoid.
When the researchers analysed the footage frame by frame, five things separated the “easy target” group from everyone else: a stride length that was unusually long or short for their height, a weight shift that moved up and down rather than side to side through the hips, movement that engaged only part of the body instead of moving as a whole, an awkward rather than smooth lift of the foot, and a general lack of coordinated, fluid rhythm. Researchers later called this “non-synchronous” movement.
It wasn’t a one-off result. It’s been retested with different methods and different groups ever since.
In 2002, researchers stripped the footage down to point-light displays, removing every visual cue except the movement itself, and found the same pattern. In 2009, the effect showed up again with ordinary students doing the rating, not just convicted offenders. In 2013, a study of 47 inmates in a maximum-security Canadian prison found the same thing, and this time the inmates could explain what they were looking at. The men who scored highest for psychopathy were also the most accurate.
People who have already been victimised once tend to carry a detectable change in how they move, and that change makes them more likely to be picked out again. Not because they’re weak. Because, as the researchers put it, the body holds on to what’s happened to it.
What’s missing from this research
None of these studies tested autistic, ADHD or dyspraxic participants. They used general members of the public and convicted offenders. The five gait markers were treated as incidental, the kind of thing that might be linked to low confidence or past trauma, but never tied to a diagnosis.
They aren’t incidental in autism. They’re well documented.
A 2021 meta-analysis combining 18 separate studies found autistic people consistently walk with a wider stance, a slower pace, a longer gait cycle, and more stride-to-stride variability than non-autistic people. That last point matters most. It’s not just that autistic gait looks different. It’s less consistent from one step to the next, which is close to a clinical description of what the offender studies call “non-synchronous” movement.
Other research has found reduced range of motion at the ankle and knee in autistic gait, along with a weaker push-off at the end of each step. Researchers tend to point to differences in the cerebellum and basal ganglia as the likely cause, the same brain regions involved in Parkinson’s-related gait problems. This isn’t a new observation either. Leo Kanner, the psychiatrist who first described autism in 1943, noted that autistic children often had a “clumsy” gait. One clinical study of older autistic children found their gait deviations were severe enough to measurably increase their risk of falls.
ADHD has a similar, less widely known connection. Up to half of children and teenagers with ADHD show some kind of motor abnormality, including problems with balance, and brain scans suggest this may be linked to atrophy in the same cerebellar regions involved in coordinating movement. One study compared ADHD children directly with children who had confirmed cerebellar damage from surgery, and found their balance problems lined up. Separate research has measured an altered pelvic tilt in ADHD gait and found ADHD children take longer, less regular strides than their peers.
Dyspraxia, known clinically as Developmental Coordination Disorder, makes the link most direct of all. An abnormal gait isn’t an occasional feature of dyspraxia. It’s part of the diagnosis itself, in adults as much as children. DCD is, at its core, a disorder of motor planning, the brain struggling to translate intention into smooth, coordinated movement. That’s a clinical description of the exact thing the victim-selection research keeps coming back to as the strongest signal of all.
These three conditions also overlap with each other far more than is generally recognised. One study screened nearly 12,000 autistic children for DCD and found only 15% had a formal diagnosis for it, while almost 87% screened as at risk on a validated test. The same body of research estimates that 30 to 55% of children with ADHD also meet the threshold for DCD. A large share of autistic and ADHD children, in other words, are also functionally dyspraxic, whether or not it’s written down anywhere.
None of the criminology studies appear to have checked for any of this. Nobody asked whether the “vulnerable” walkers in their footage were autistic, had ADHD, or were dyspraxic.
The pattern shows up elsewhere too
A separate strand of research, with nothing to do with predatory crime, points in the same direction.
A study of more than 4,000 eight-year-olds looked at which autism-related traits predicted being bullied. Out of everything measured, the single strongest predictor, flagged by both parents and teachers, was having “clumsy, ill-coordinated, ungainly, awkward movements.” Unusual facial expressions and posture didn’t predict bullying in the same study. Movement did.
That’s a different age group and a different kind of harm to the Grayson and Stein research. But it’s the same signal being picked up by a different set of observers, arriving at the same answer: visibly atypical movement draws targeting.
It also lines up with how the law already treats this in England and Wales. Crown Prosecution Service guidance on disability hate crime draws a clear distinction between offences motivated by hostility towards disability, and a separate category: offences where the victim was targeted simply because the offender saw them as vulnerable, with no hostility involved at all. The CPS treats the second category as an aggravating factor for sentencing in its own right.
Government figures cited in Parliament put the proportion of young people with what’s officially termed a “social or behavioural impairment”, a category covering autism, ADHD and Asperger’s, who had been a crime victim in the past year at 35%, against 12% for their non-disabled peers. Surveys of people with learning disabilities have found even higher rates, with some putting the proportion who’ve experienced a hate crime at close to three in four.
None of these figures prove gait is the mechanism. But they’re consistent with one.
What this isn’t saying
This isn’t a finding that neurodivergent gait causes victimisation. No study on gait and victim selection has tested autistic, ADHD or dyspraxic people directly as far as I’m currently aware. This article is placing two separate fields of research next to each other, not reporting a result either field has published. Treat it as a hypothesis worth investigating properly, not a settled conclusion.
It’s also not an argument that responsibility shifts onto the person targeted. Every study cited here, including the original 1981 paper, frames vulnerability cues as something predators exploit, with responsibility for the offence sitting entirely with the offender. The CPS guidance is built on exactly that distinction. Perceived vulnerability explains why someone might be selected. It explains nothing about blame.
Gait in autism, ADHD and dyspraxia comes from how the brain plans and controls movement. It isn’t posture, confidence or attitude, and it can’t be fixed by trying harder to “walk taller.” Advice along those lines, common in self-defence and personal safety content, doesn’t apply in the same way to someone whose gait differences are neurological rather than habitual.
What public services could actually do
There is, however, a difference between telling someone to “walk taller” and offering structured support to build coordination, balance and motor control, the kind of input that already exists in clinical practice and has trial evidence behind it.
Occupational therapy and physiotherapy programmes built specifically for motor coordination difficulties, rather than generic exercise advice, have shown measurable results. A randomised waitlist-controlled trial of an approach called Cognitive Orientation to daily Occupational Performance found significant improvements in motor performance and movement quality in autistic children with DCD, with most of the gains still holding three months after treatment ended. Other controlled trials of structured motor-skill occupational therapy in autistic children have found similar improvements in coordination and functional mobility. None of this is hypothetical or alternative medicine. It’s mainstream paediatric occupational therapy, already used to treat DCD on its own, just rarely connected explicitly to the question of physical vulnerability.
The same research notes that only about half of children with ADHD who have motor difficulties ever receive motor-based treatment for them, because ADHD assessment tends to focus on attention and hyperactivity and the coordination side gets overlooked. Given that DCD is present at clinical levels in the large majority of autistic children and a significant minority of children with ADHD, this is a sizeable population receiving a diagnosis for one condition while a related, treatable physical difficulty goes unaddressed.
Access is the more basic problem. The Children’s Commissioner for England has reported children waiting upwards of two and a half years from referral to autism diagnosis in some areas, with similarly long waits for ADHD, before any therapeutic support, motor or otherwise, is even considered. Coordination and balance work is not currently treated as a standard, automatic part of an autism or ADHD care pathway, despite both conditions carrying a well-documented motor component from the point of diagnosis.
If a public body has a duty of care toward a group it already knows is at elevated risk of being targeted by violent or exploitative offenders, prevention has to include the things that are actually within that body’s control. Reducing waiting times for occupational therapy and physiotherapy referrals, building motor coordination support into standard autism and ADHD care pathways rather than leaving it to be requested separately, and training frontline safeguarding staff to recognise gait-related vulnerability as a genuine, addressable risk factor rather than an unchangeable trait would all sit squarely within that duty. None of it requires new legislation. It requires treating a documented physical risk factor as seriously as any other.
A YouTube video by ThatGearGuy, drawing on his 23 years in professional security, recently brought the Grayson and Stein research to wider attention and prompted the writing of this piece. No affiliation is claimed with the channel.
Further reading
- The Cheshire West Ruling Shows How Disabled People Lose Liberty Quietly
- FOI reveals disabled job applicants lost in recruitment data gap
Sources
- Grayson, B. and Stein, M.I. (1981). Attracting Assault: Victims’ Nonverbal Cues. Journal of Communication, 31, 68-75. https://doi.org/10.1111/j.1460-2466.1981.tb01206.x
- Gunns, R.E., Johnston, L. and Hudson, S.M. (2002). Victim Selection and Kinematics: A Point-Light Investigation of Vulnerability to Attack. Journal of Nonverbal Behavior, 26, 129-158. https://link.springer.com/article/10.1023/A:1020744915533
- Wheeler, S., Book, A. and Costello, K. (2009). Psychopathic Traits and Perceptions of Victim Vulnerability. Criminal Justice and Behavior, 36, 635-648. https://doi.org/10.1177/0093854809333958
- Book, A., Costello, K. and Camilleri, J.A. (2013). Psychopathy and Victim Selection: The Use of Gait as a Cue to Vulnerability. Journal of Interpersonal Violence, 28, 2368-2383. https://doi.org/10.1177/0886260512475315
- Dark Tetrad and gait-based victim selection study (2018). https://www.sciencedirect.com/science/article/abs/pii/S0191886918304896
- Lum, J.A.G. et al. (2021). Meta-Analysis Reveals Gait Anomalies in Autism. Autism Research, 14, 733-747. https://doi.org/10.1002/aur.2443
- Kindregan, D., Gallagher, L. and Gormley, J. (2015). Gait Deviations in Children with Autism Spectrum Disorders: A Review. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4398922/
- Clinical gait analysis study, older autistic children and fall risk. https://www.sciencedirect.com/science/article/pii/S2666337623000793
- Postural and gait performance study, ADHD children versus children with cerebellar lesions. https://pubmed.ncbi.nlm.nih.gov/18963991/
- Increased Anterior Pelvic Angle in ADHD gait study. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0170096
- Gait and gross motor skills study in ADHD-CT children. https://pmc.ncbi.nlm.nih.gov/articles/PMC9985067/
- Study on motor abnormalities and grey matter volume in ADHD and autism, including DCD comorbidity figures. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8129495/
- Junttila, M. et al. (2023). The traits of Autism Spectrum Disorder and bullying victimization in an epidemiological population. European Child & Adolescent Psychiatry. https://doi.org/10.1007/s00787-023-02228-2
- Crown Prosecution Service, Investigating and Prosecuting Disability Hate Crime: Best Practice. https://www.cps.gov.uk/publication/investigating-and-prosecuting-disability-hate-crime-best-practice
- Hansard, House of Commons debate on CPS and Disability Hate Crime, 2016. https://hansard.parliament.uk/commons/2016-11-08/debates/1ED75BC0-7686-41FD-B8B4-26B110F25AAC/CPSAndDisabilityHateCrime
- Mental Health Foundation, A Life Without Fear? report on learning disability hate crime. https://www.mentalhealth.org.uk/about-us/news/new-report-shows-people-learning-disabilities-are-high-risk-targeting-hate-crime-yet-remain
- Cengiz, E. et al. Effectiveness of Cognitive Orientation to daily Occupational Performance (CO-OP) for autistic children with DCD. https://pmc.ncbi.nlm.nih.gov/articles/PMC11695746/
- Effectiveness of CO-OP intervention in improving motor skills of children with DCD: a randomized waitlist-control trial. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9082975/
- Children’s Commissioner for England. Waiting times for assessment and support for autism, ADHD and other neurodevelopmental conditions. https://www.childrenscommissioner.gov.uk/resource/waiting-times-for-assessment-and-support-for-autism-adhd-and-other-neurodevelopmental-conditions/


Be First to Comment