Six national bodies didn’t identify a legal, regulatory or clinical THC ceiling for prescribed cannabis flower.
By The Reasonable Adjustment
British private medical cannabis clinics that apply fixed THC ceilings appear to be doing so under their own prescribing policies, rather than a maximum percentage set by law or national guidance.
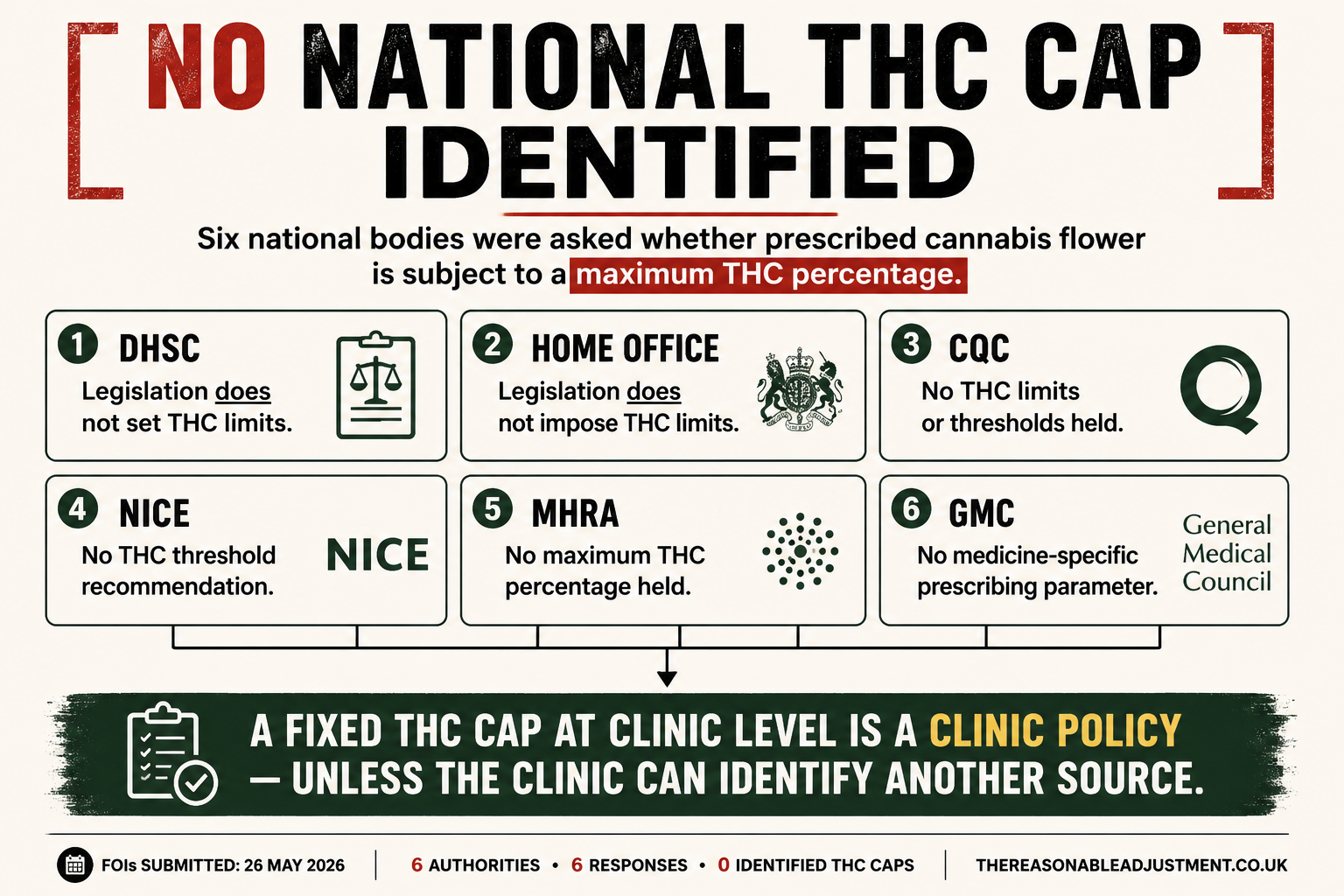
Six national bodies were asked whether they held guidance, policy or other recorded information setting a maximum THC percentage for prescribed cannabis flower. The requests covered common thresholds including 20%, 22%, 25%, 26%, 28% and 30%, along with any additional approval, risk assessment or governance expected when higher-THC flower is prescribed.
None identified a national THC cap.
The requests were sent to the Department of Health and Social Care, Home Office, Care Quality Commission, National Institute for Health and Care Excellence, Medicines and Healthcare products Regulatory Agency and General Medical Council.
The Department of Health and Social Care said it didn’t hold recorded information setting, recommending, endorsing or discussing a maximum THC percentage for prescribed cannabis-based products for medicinal use. It also confirmed that the legislation governing CBPMs “does not set THC limits”, with treatment decisions left to prescribers acting within the law, professional standards and relevant clinical guidance.
The Home Office gave the same answer on the legal position. It said CBPM legislation doesn’t impose THC limits, while prescribing practice, dosage and routes of administration sit outside its remit.
Neither department identified a legal rule requiring prescribed cannabis flower to remain below a particular THC percentage.
No national clinical or regulatory threshold identified
The Care Quality Commission said it didn’t hold information on THC percentage limits, caps or thresholds. Its response pointed instead to NHS England guidance on multidisciplinary clinical decision-making, saying providers should follow that guidance regardless of the strength or formulation of the cannabis-based medicine.
NICE said its guideline on cannabis-based medicinal products, NG144, doesn’t make recommendations on THC percentage limits or thresholds. It also said it held no information on how private clinics are expected to justify, review, audit or document decisions involving higher-THC flower.
NICE’s guidance formally covers NHS and commissioned social-care settings. Private providers may choose to follow it, but NICE said its recommendations don’t formally apply to private clinics.
The MHRA said it held no information on a maximum THC percentage in unlicensed CBPM products. That is directly relevant to prescribed cannabis flower, much of which is supplied as an unlicensed medicine.
The GMC said it didn’t hold information within scope of the request. It explained that it sets professional standards for doctors, but doesn’t regulate cannabis-based medicinal products or set clinical prescribing parameters for particular medicines.
The six replies cover health policy, controlled-drug law, healthcare inspection, medicines regulation, clinical guidance and medical professional standards. None pointed to a national THC ceiling.
Clinic policy should be described as clinic policy
The FOIs weren’t asking whether THC strength is clinically irrelevant. It plainly isn’t. A patient’s symptoms, previous cannabis use, treatment response, side effects, dose, mental-health history and wider circumstances may all affect what a specialist is prepared to prescribe.
A clinic may also decide to run a cautious prescribing policy. It may choose not to prescribe flower above a particular percentage, require senior review for some products, or take a more restrictive approach than another provider.
But a fixed clinic rule isn’t the same as a national requirement.
Where a patient is told that a product can’t be prescribed because it exceeds 20%, 22%, 25% or another stated limit, the clinic should be clear about what sits behind that decision. Is it an individual clinical assessment? A written clinic-wide policy? A medical director’s instruction? An insurer requirement? A governance decision based on the clinic’s own reading of the available evidence?
Those aren’t semantic differences. They determine whether a patient is being told that a product is prohibited nationally, ruled out by the clinic, or considered unsuitable in their own case.
A clinic may have a defensible reason for its threshold. The six FOI responses don’t establish that every cap is unsound, and they don’t show that every clinic uses one. They do establish that the national bodies approached for this investigation didn’t identify a legal, regulatory or clinical THC ceiling for prescribed cannabis flower.
That leaves clinics using fixed limits with a straightforward responsibility: explain their own policy accurately, rather than allowing patients to assume it comes from government, regulators or national prescribing guidance.
Further reading
- Why Medical Cannabis Repeat Orders Can Be So Confusing for Patients
- Why Is West Lancashire Treating Medical Cannabis Like a Police Matter?
- Prescribed Medical Cannabis at Events, Gigs and Festivals in the UK
- NPCC Medical Cannabis Guidance
Sources
The six Freedom of Information requests were submitted through WhatDoTheyKnow on 26 May 2026.
- Care Quality Commission response
- General Medical Council response
- Department of Health and Social Care response
- Home Office response
- MHRA response
- NICE response
- Full WhatDoTheyKnow batch
Be First to Comment